Cognitive decline strikes in many different ways, including pathologies such as Alzheimer’s Disease (AD), but in the end many ways of describing how the brain has declined are related to breakdowns in our brain and body’s ability to properly metabolize energy. If we can target the metabolism in the body and brain and rejuvenate and/or reactivate it, there is potential to mitigate and even reverse the decline induced by it.
A great group out of a great anti-aging research institute, the Buck Institute for Research on Aging, has come up with a novel protocol for enhancing metabolism in the brain that can objectively combat the decline caused by Alzheimer’s disease. Out of 10 patients in the trial who had Alzheimer’s disease or other types of cognitive impairment, 9 of them were able to make significant and objective improvements. Six of the patients had previously had to discontinue their jobs or were having great difficulty at work, and all of them were able to return to work or improved greatly. The results were seen within 3-6 months of the protocol and continued through to the longest checkup, which was 2.5 years after beginning the protocol.
Current therapies for Alzheimer’s and other neurodegenerative diseases typically focus on a single type of therapy and hoping that it will completely reverse such a damaging disease. In my opinion, and the opinion of the authors of this study, this is a major failure and embarrassment to the medical establishment. It is unresonable to think that a single intervention can reverse a disease and the decline caused by a multitude of factors. In the case of Alzheimer’s there is actually not a lot of research on combination therapies, while at the same time the last few decades have revealed that there are extensive molecular functions involved in AD. It is from this perspective that the authors of the study sought to test a network-based therapeutic approach instead of a single target-based approach.
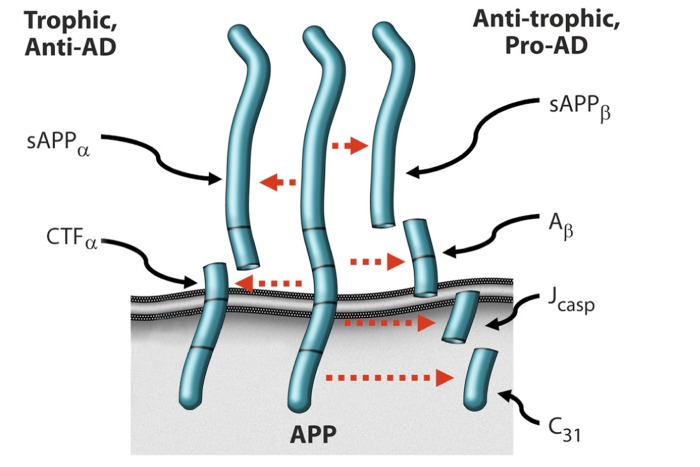
Without getting too deep into the heavy scientific language (you can read the full paper here), the scientists looked at interventions on a wide range of targets, from amyloid-β (Aβ) and tau plaques, to inflammatory mediators, metabolism factors, regulatory pathways, and neurotransmitters. They eventually settled on an advanced model that links AD to an imbalance in endogeneous plasticity signaling in the brain where β-amyloid precursor protein (APP) is the signaling agent. There are a number of signaling molecules in the brain that can alter the neurite-retracting and neurite-extending peptides, and when this balance is in favor of the neurite-retracting peptides, AD is worse. On top of that, these switches seem to act together in what the researches call molecular switches, and one switch can then cause a cascade of positive feedback that reverses some symptoms of AD.
In mouse models, genes that signal APP seems to be manipulated fairly easily through the targeting of specific genes, however in humans a large proportion of patients with AD do not have a single gene that can alter APP or other AD-related genes. Due to the many inputs to APP signaling balance in humans (e.g. estrogen, netrin-1, Aβ, etc) and the minimal success from therapeutic agents in altering this signaling alone, they decided upon a system, rather than a single targeted agent to try and find success combating AD. The scientists are hoping to correct the ratio of synapse destruction to synapse creation (synaptoblastic:synaptoclastic balance).

The basic system is as follows:
1. The goal is not to simply try and normalize metabolic parameters, but to optimize them. An example they use is homocysteine, for which a “normal” limit in most considerations is 12 μmol/l, however it was well documented to be suboptimal, especially in terms of AD mitigation. They make similar arguments for many other metabolic parameters.
2. Based on the hypothesis that AD results from an imbalance in the brain’s extensive plasticity network, therapy should focus on addressing as many of the network components as possible, because the combination can have an effect greater than any of the individual monotherapies alone.
3. This protocol is based on the idea that the effects of AD are related to its effects on the network of systems in the body and that once a certain threshold is reached and enough of the components of the network are impacted, the AD can be reversed. This means that each patient is not required to follow every step of the protocol, but enough to make a difference to the network.
4. This approach to combating AD is personalized and based on lab values affecting the plasticity network so as physiological data points are analyzed, different interventions may be prioritized in the program.
5. The program is iterative so that there is a continued optimization over time.
6. For each component in the network, the goal is to address it as far upstream as possible.
Now that you’ve got the theoretical parts of the system, here is a breakdown of the actual Therapeutic System 1.0 used in these patients. Remember that not all patients did all of the metrics.
Table 1. Therapeutic System 1.0
| Goal | Approach | Rationale and References | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Optimize diet: minimize simple CHO, minimize inflammation. | Patients given choice of several low glycemic, low inflammatory, low grain diets. | Minimize inflammation, minimize insulin resistance. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Enhance autophagy, ketogenesis | Fast 12 hr each night, including 3 hr prior to bedtime. | Reduce insulin levels, reduce Aβ. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Reduce stress | Personalized—yoga or meditation or music, etc. | Reduction of cortisol, CRF, stress axis. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Optimize sleep | 8 hr sleep per night; melatonin 0.5mg po qhs; Trp 500mg po 3x/wk if awakening. Exclude sleep apnea. | [36] | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Exercise | 30-60′ per day, 4-6 days/wk | [37, 38] | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Brain stimulation | Posit or related | [39] | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Homocysteine <7 | Me-B12, MTHF, P5P; TMG if necessary | [40] | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Serum B12 >500 | Me-B12 | [41] | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| CRP <1.0; A/G >1.5 | Anti-inflammatory diet; curcumin; DHA/EPA; optimize hygiene | Critical role of inflammation in AD | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Fasting insulin <7; HgbA1c <5.5 | Diet as above | Type II diabetes-AD relationship | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Hormone balance | Optimize fT3, fT4, E2, T, progesterone, pregnenolone, cortisol | [5, 42] | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| GI health | Repair if needed; prebiotics and probiotics | Avoid inflammation, autoimmunity | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Reduction of A-beta | Curcumin, Ashwagandha | 43–45 | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Cognitive enhancement | Bacopa monniera, MgT | [46, 47] | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| 25OH-D3 = 50-100ng/ml | Vitamins D3, K2 | [48] | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Increase NGF | H. erinaceus or ALCAR | [49, 50] | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Provide synaptic structural components | Citicoline, DHA | [51]. | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Optimize antioxidants | Mixed tocopherols and tocotrienols, Se, blueberries, NAC, ascorbate, α-lipoic acid | [52] | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Optimize Zn:fCu ratio | Depends on values obtained | [53] | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Ensure nocturnal oxygenation | Exclude or treat sleep apnea | [54] | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Optimize mitochondrial function | CoQ or ubiquinol, α-lipoic acid, PQQ, NAC, ALCAR, Se, Zn, resveratrol, ascorbate, thiamine | [55] | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Increase focus | Pantothenic acid | Acetylcholine synthesis requirement | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Increase SirT1 function | Resveratrol | [32] | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| Exclude heavy metal toxicity | Evaluate Hg, Pb, Cd; chelate if indicated | CNS effects of heavy metals | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| MCT effects | Coconut oil or Axona | [56] | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
| CHO, carbohydrates; Hg, mercury; Pb, lead; Cd, cadmium; MCT, medium chain triglycerides; PQQ, polyquinoline quinone; NAC, N-acetyl cysteine; CoQ, coenzyme Q; ALCAR, acetyl-L-carnitine; DHA, docosahexaenoic acid; MgT, magnesium threonate; fT3, free triiodothyronine; fT4, free thyroxine; E2, estradiol; T, testosterone; Me-B12, methylcobalamin; MTHF, methyltetrahydrofolate; P5P, pyridoxal-5-phosphate; TMG, trimethylglycine; Trp, tryptophan | |||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||||
You can read the case studies of the people this worked on by checking the full study below.
Full text study -> Reversal of cognitive decline: A novel therapeutic program
